

Best Probiotic Strains for Oral Health: Complete Guide 2026

Oral health is far more complex than brushing and flossing. Beneath the surface of every smile lives a dynamic ecosystem of over 700 bacterial species — and the balance between them determines whether your teeth and gums stay healthy or deteriorate over time. Understanding the best probiotic strains for oral health has become one of the most important advances in preventive dentistry over the past decade.
For most of history, dental care focused on eliminating bacteria. Antiseptic mouthwashes, antibiotics, and fluoride treatments all aim to reduce microbial populations. However, this approach has a fundamental limitation: it destroys beneficial bacteria alongside harmful ones. According to research published in Frontiers in Microbiology (2024), tooth decay and gum disease still affect over 90% and 50% of American adults respectively — despite decades of conventional treatment.
A growing body of clinical evidence suggests that introducing targeted probiotic bacteria into the oral cavity may offer a more sustainable solution. Rather than eliminating all bacteria, oral probiotics work by restoring microbial balance — a strategy aligned with how healthy mouths naturally protect themselves. In this complete scientific guide, you will discover which probiotic strains are best supported by research, how they work inside your mouth, what conditions they address, and how to evaluate probiotic products intelligently.
💡 Want to understand how specific probiotic strains protect your teeth and gums? Continue reading this evidence-based guide — you will find strain-by-strand scientific breakdowns, clinical study summaries, and practical guidance for choosing the right oral probiotic in 2026.
What Are Oral Probiotic Strains and Why Do They Matter?
The term “probiotic” was formally defined by the World Health Organization in 2001 as “live microorganisms which, when administered in adequate amounts, confer a health benefit on the host.” Most consumers associate probiotics with digestive health. However, the oral cavity is arguably an even more logical environment for probiotic therapy — because nearly all common oral diseases originate from microbial imbalance.
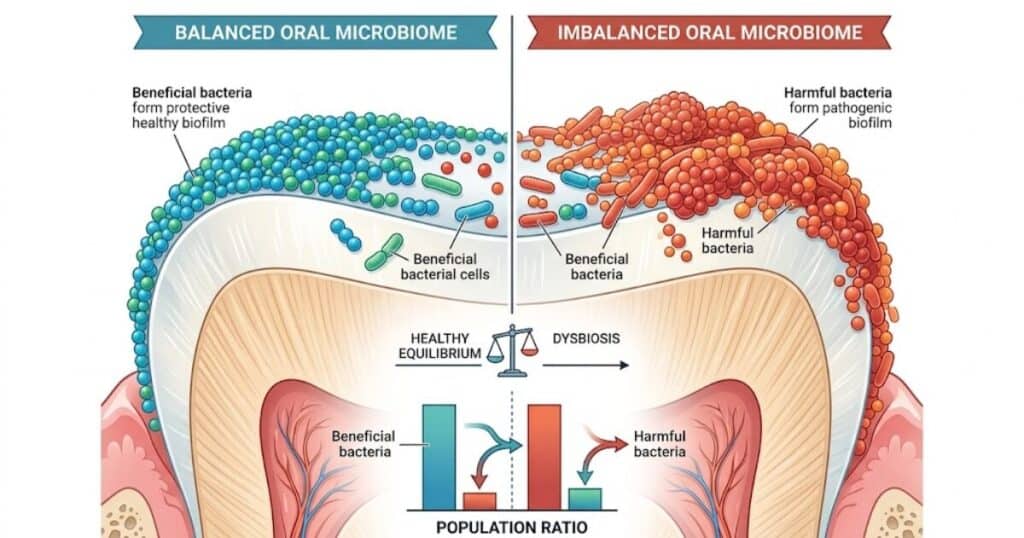
When harmful bacteria overpopulate the mouth, they produce acids that erode enamel, volatile sulfur compounds that cause bad breath, and inflammatory signals that attack gum tissue. The primary driver of cavities is an overgrowth of Streptococcus mutans, while periodontitis — advanced gum disease — is closely linked to the proliferation of Porphyromonas gingivalis and Tannerella forsythia. Probiotic strains do not simply “add good bacteria.” They actively compete with pathogens for nutrients, attachment sites, and resources — a process known as competitive exclusion.
Not all probiotics are equally suited for oral use. A strain isolated from the human intestine behaves very differently from one isolated from healthy gum tissue. Effective oral probiotic strains must be able to survive the oral environment, adhere to oral surfaces, and produce metabolites that specifically inhibit oral pathogens. This is why strain specificity — not just species or genus — is critical when evaluating any probiotic product for dental health.
How Probiotics Differ From General Gut Supplements
General gut probiotics — such as Lactobacillus acidophilus commonly found in yogurt — are optimized for intestinal colonization. They may pass through the mouth, but they do not establish meaningful populations in oral tissues. In contrast, true oral probiotic strains are isolated from healthy human mouths, adapted to survive salivary flow and oral pH, and demonstrated to produce measurable benefits in clinical dental studies.
What Makes a Probiotic Strain Effective for the Mouth?
According to a 2024 systematic review in Frontiers in Microbiology, effective oral probiotic strains share several characteristics: they originate from the oral cavity of healthy subjects, produce antimicrobial metabolites such as hydrogen peroxide or bacteriocins, survive in the presence of saliva, and adhere strongly to tooth or gum surfaces. Safety profiles and the absence of antibiotic resistance genes are also mandatory criteria for responsible inclusion in probiotic products.
The Science of the Oral Microbiome Explained
The oral microbiome is one of the most diverse microbial communities in the human body. In a healthy adult, genera such as Streptococcus, Rothia, Neisseria, Veillonella, and Actinomyces dominate. Dysbiosis — an imbalance in this community — is the root cause of most oral diseases. Probiotic therapy aims to restore this balance rather than achieve sterility, which is both impossible and biologically counterproductive.
How Do Oral Probiotics Work Inside Your Mouth?
Understanding the mechanisms behind oral probiotics helps explain why certain strains outperform others — and why not all “probiotic” products marketed for dental health deliver real results. Research identifies three primary mechanisms through which oral probiotic strains confer health benefits: competitive interactions, antimicrobial production, and immune modulation.
Colonization: How Beneficial Bacteria Establish in Oral Tissues
Probiotic bacteria must first colonize oral surfaces to exert any benefit. Streptococcus species — natural early colonizers of tooth enamel — produce adhesins that allow them to bind tightly to the salivary pellicle, a protein film that coats teeth. This strong attachment is critical because saliva flow and eating create significant shearing forces. Probiotic strains with high adhesion capacity, such as Streptococcus salivarius and S. oralis, are far more likely to establish lasting populations than transient visitors.
Competitive Exclusion: Crowding Out Harmful Bacteria
Once established, probiotic bacteria occupy the same ecological niches as oral pathogens. Streptococcus rattus JH145, for example, colonizes the same sites on tooth surfaces as the cavity-causing S. mutans — but unlike S. mutans, it does not produce lactic acid, making it non-cariogenic. This competitive exclusion strategy reduces the pathogen’s ability to cause harm without requiring the elimination of the entire bacterial community.
Anti-Inflammatory Mechanisms of Oral Probiotic Strains
Several oral probiotic strains downregulate proinflammatory cytokines in gum tissue. A 2021 study published in BMC Oral Health demonstrated that Streptococcus salivarius strains significantly reduced immune activation triggered by periodontal pathogens. This anti-inflammatory effect is particularly relevant for patients with gingivitis or early-stage periodontitis, where chronic inflammation drives tissue destruction.
How Probiotics Influence Salivary pH and Enamel Protection
Cavity formation requires an acidic oral environment. Commensal oral streptococci contain the arginine deiminase system (ADS), which converts arginine to ammonia — raising local pH and creating an alkaline environment hostile to cariogenic bacteria. Prebiotics such as arginine and urea further support this mechanism. Maintaining a neutral or slightly alkaline oral pH is one of the most underappreciated strategies for long-term enamel protection.
Best Probiotic Strains for Teeth and Gums: Scientific Breakdown
This is the core of what most consumers need — and what most probiotic marketing glosses over. Probiotic benefits are strain-specific, not species-specific. Two products may both contain Lactobacillus reuteri but deliver entirely different clinical outcomes depending on which strain is included. Below is a research-grounded breakdown of the most clinically supported oral probiotic strains available in 2026.
| Probiotic Strain | Primary Benefit | Mechanism | Clinical Support |
|---|---|---|---|
| S. salivarius BLIS M18 | Cavity & plaque control | Bacteriocin production | Strong (multiple RCTs) |
| S. salivarius BLIS K12 | Fresh breath, throat health | Lantibiotic production | Strong (multiple RCTs) |
| S. oralis KJ3 | Gum pathogen inhibition | H₂O₂ production | Moderate |
| L. paracasei | Plaque biofilm reduction | S. mutans inhibition | Moderate |
| L. reuteri DSM 17938 | Gum inflammation | Immune modulation | Mixed evidence |
| B. lactis BL-04 | Immune support | Systemic immune signaling | Indirect / emerging |
| B. coagulans IS2 | S. mutans reduction | Unknown mechanism | Preliminary |
Lactobacillus Paracasei: Gum Defense and Plaque Resistance
Lacticaseibacillus paracasei strains SD1 and ET-22 have demonstrated the ability to reduce S. mutans concentrations in saliva and inhibit biofilm formation in randomized controlled trials. A 2023 study in Nutrients found that L. paracasei ET-22 significantly suppressed dental caries-associated bacteria by targeting plaque microbiota. However, most research remains preliminary, and long-term placebo-controlled trials are still limited.
Lactobacillus Reuteri: Anti-Inflammatory Properties for Gums
Limosilactobacillus reuteri strains DSM 17938 and ATCC PTA 5289 are among the most studied oral probiotic candidates. Some studies report improvements in gingival health and reductions in periodontal pathogen levels following use. However, the European Food Safety Authority issued a 2020 statement indicating that current evidence is insufficient to confirm a direct gum health benefit from these strains alone. Results are therefore promising but should be interpreted with appropriate caution.
Bifidobacterium Lactis BL-04: Immune Support and Oral Barrier
Bifidobacterium lactis BL-04 is primarily a gut probiotic with emerging research in oral immunity. It has not been isolated from healthy oral tissues and currently lacks strain-specific clinical evidence for direct oral cavity benefits. Its inclusion in oral probiotic products is largely based on general immunological benefits rather than targeted dental research. Consumers should be aware of this distinction when evaluating products that list this strain.
Streptococcus Salivarius BLIS M18: Cavity and Plaque Control
Streptococcus salivarius M18 is one of the most scientifically robust oral probiotic strains available. Isolated from the oral cavity of a healthy adult, it produces three distinct bacteriocins — salivaricin A2, salivaricin 9, and salivaricin M — that inhibit multiple oral pathogens. A randomized controlled trial by Di Pierro et al. (2015) demonstrated significant reductions in caries risk scores in children after 90 days of supplementation. Clinical studies also confirm reductions in the abundance of periodontal pathogens.
Streptococcus Salivarius K12: Fresh Breath and Throat Health
S. salivarius K12 is the gold-standard strain for halitosis management. Isolated from a child’s saliva, it produces salivaricin A and salivaricin B — lantibiotics that directly inhibit Fusobacterium nucleatum and other volatile sulfur compound (VSC)-producing bacteria. A 2020 study in Clinical and Experimental Dental Research confirmed that the combination of K12 and M18 significantly reduces VSC levels. Beyond oral health, K12 is also well studied for ear, nose, and throat applications.
Lactobacillus Rhamnosus: Reducing Oral Pathogen Load
Lactobacillus rhamnosus strains have shown some capacity to inhibit S. mutans adhesion in vitro and reduce caries incidence in some pediatric studies. However, as with other Lactobacillus species, their status as transient rather than permanent oral colonizers limits their long-term effectiveness as standalone oral health probiotics. They are better considered adjunctive rather than primary oral probiotic strains.
Bacillus Coagulans: Stability and Bioavailability Advantages
Bacillus coagulans Unique IS2 has one notable advantage over other oral probiotics: its spore-forming nature makes it exceptionally stable at room temperature without refrigeration. A 2020 double-blind, placebo-controlled trial found significant reductions in salivary S. mutans and Lactobacillus levels after 14 days of use. However, the mechanism of action has not been identified, and additional studies are needed before this strain can be considered well-validated for oral care.
⭐ Scientific note: Unlike mouthwashes that eliminate all bacteria — including beneficial ones — the best oral probiotic strains were designed to repopulate the mouth with specific bacteria that naturally compete with the pathogens responsible for cavities, gum disease, and bad breath. This represents a paradigm shift: from elimination to restoration.
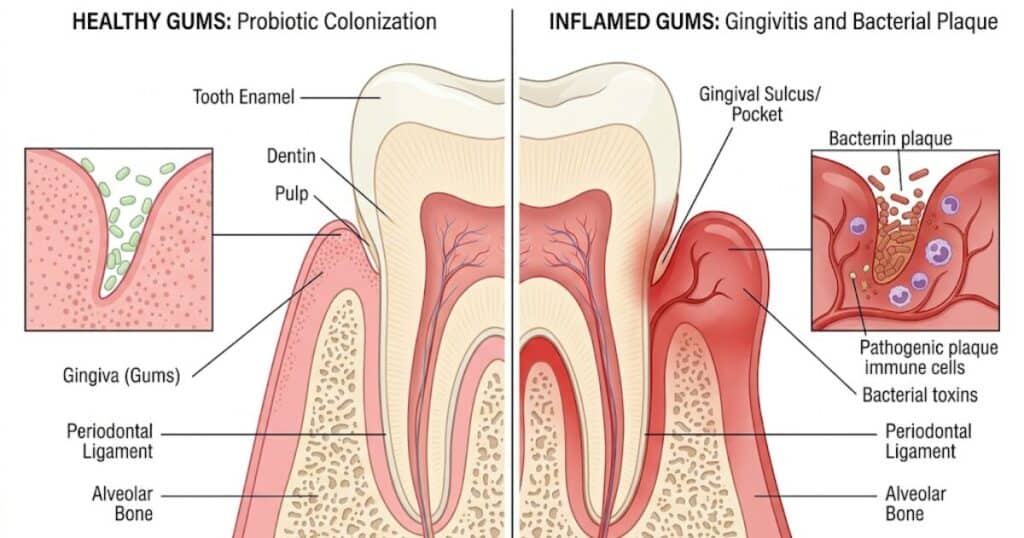
Which Probiotic Strains Benefit Gum Disease and Inflammation?
Gum disease — from mild gingivitis to advanced periodontitis — affects more than half of adults over 30. It is driven by dysbiosis of the subgingival microbiome, where pathogens like Porphyromonas gingivalis, Tannerella forsythia, and Aggregatibacter actinomycetemcomitans overwhelm the commensal population. Probiotic strains that inhibit these specific pathogens offer a genuine therapeutic avenue.
Probiotics and Gingivitis: What Clinical Studies Show
A systematic review published in BMC Oral Health found that adjunctive use of probiotic lozenges significantly reduced bleeding on probing (BOP) — a key clinical marker of gum inflammation — compared to placebo. L. reuteri containing lozenges showed statistically significant decreases in bleeding scores within four weeks in several Australian and European trials. S. salivarius M18 has similarly demonstrated reductions in periodontal pathogen counts in randomized controlled trials.
Can Probiotics Reduce Periodontitis Progression?
Periodontitis involves irreversible destruction of bone and connective tissue around teeth. While probiotics cannot reverse existing damage, emerging evidence suggests they may slow progression. A clinical trial by Teughels et al. found that adjunctive L. reuteri lozenges improved pocket probing depths in chronic periodontitis patients receiving standard scaling and root planing. Probiotics are best positioned as adjunctive therapy — complementing professional treatment, not replacing it.
Reducing Bleeding Gums: Evidence-Based Strain Recommendations
For patients specifically targeting gum bleeding, the strains with the strongest evidence are S. salivarius M18 (bacteriocin-mediated pathogen inhibition), L. reuteri DSM 17938 (anti-inflammatory immune modulation), and the S. oralis KJ3 / S. uberis KJ2 combination (hydrogen peroxide production against anaerobic periodontal pathogens). Consistent daily use for at least four to six weeks is necessary to observe measurable clinical changes.
Oral Probiotics for Halitosis: Strains That Fight Bad Breath
Chronic bad breath — halitosis — affects approximately 25% of the global population and is a significant source of social anxiety. In most cases, the root cause is not poor hygiene but rather an overpopulation of anaerobic bacteria in the posterior tongue, gingival crevices, and periodontal pockets.
Root Causes of Chronic Bad Breath in the Microbiome
Bacteria such as Fusobacterium nucleatum, Treponema denticola, and Tannerella forsythia metabolize sulfur-containing amino acids to produce hydrogen sulfide and methyl mercaptan — the compounds responsible for the characteristic odor of bad breath. These volatile sulfur compounds (VSCs) are produced in anaerobic (oxygen-poor) environments, which is why tongue coating and deep gum pockets are primary sources. Standard mouthwashes mask VSCs temporarily but do not alter the underlying microbial population.
How BLIS K12 and M18 Target Odor-Causing Bacteria
S. salivarius K12 is specifically adapted to colonize the dorsum of the tongue — the primary reservoir of VSC-producing bacteria. Its lantibiotics directly inhibit the growth of anaerobic pathogens responsible for odor production. In combination with M18, which targets subgingival pathogens, the two strains provide comprehensive coverage of the oral cavity. A 2020 in vitro study confirmed that K12 and M18 together significantly inhibit VSC-producing bacteria at concentrations achievable through standard lozenge dosing.
Clinical Evidence on Probiotics and Halitosis Reduction
A 2023 randomized controlled trial published in Frontiers in Microbiology found that Weissella cibaria CMU — a newer probiotic candidate — improved halitosis scores significantly compared to placebo. Earlier studies on S. salivarius K12 consistently show reductions in organoleptic breath scores within two to four weeks of use. The evidence base for probiotics in halitosis management is now considered sufficient to warrant clinical recommendation as an adjunctive strategy.
Probiotics and Tooth Enamel: Can Good Bacteria Strengthen Teeth?
One of the most underexplored frontiers in oral probiotic research is enamel protection and remineralization. Enamel — the hardest substance in the human body — cannot regenerate once lost. However, the oral environment can be actively managed to slow or prevent demineralization.
How Lactic Acid Bacteria Influence Enamel Remineralization
A critical distinction exists between cariogenic Lactobacillus species — which produce lactic acid and erode enamel — and commensal streptococci that produce alkali through the arginine deiminase pathway. The commensal strains raise local oral pH, creating conditions in which calcium and phosphate ions can reprecipitate into demineralized enamel. This natural remineralization process is undermined by dietary acids and cariogenic bacteria. Supporting it through targeted probiotics is an emerging but scientifically sound strategy.
Malic Acid as a Natural Whitening and Enamel Support Agent
Malic acid — found naturally in strawberries and apples — acts as a salivary stimulant and mild chelating agent. It supports enamel by stimulating saliva flow (which buffers oral acids and delivers calcium and phosphate) and by gently removing surface stains without abrasion. Some probiotic formulations, including ProDentim, incorporate malic acid specifically for this dual purpose. The whitening effect is gradual and cosmetic, not structural — an important distinction for realistic expectations.
Tricalcium Phosphate: Structural Reinforcement for Teeth
Tricalcium phosphate (TCP) is a bioavailable form of calcium that provides raw material for enamel remineralization. When combined with fluoride or used in probiotic formulations, TCP has shown measurable increases in enamel microhardness in laboratory studies. Its inclusion in oral health supplements reflects an evolving understanding that enamel support is not limited to fluoride — mineral availability and oral pH work in concert.
Prebiotics and Postbiotics: Supporting Your Oral Probiotic Strains
Probiotics do not operate in isolation. Prebiotics — substrates that feed beneficial bacteria — and postbiotics — bioactive compounds produced by probiotic bacteria — are increasingly recognized as essential components of a comprehensive oral health strategy.
What Is Inulin and How It Feeds Oral Probiotics
Inulin is a naturally occurring prebiotic fiber that selectively stimulates the growth of beneficial bacteria without providing fermentable substrate for cariogenic species like S. mutans. In the oral cavity, inulin supports the proliferation of probiotic strains without raising the risk of acid production. It is one of the few prebiotics with a sufficiently specific activity profile to be considered appropriate for oral cavity supplementation.
Postbiotic Metabolites That Protect Gum Tissue
Postbiotics are compounds produced by probiotic bacteria that exert health effects independently of the live bacteria themselves. Hydrogen peroxide produced by S. oralis KJ3 and bacteriocins from S. salivarius strains are examples of postbiotic metabolites with measurable antimicrobial and whitening effects. Research published in Aging (2022) demonstrated that heat-killed probiotic preparations — delivering only the postbiotic fraction — could still inhibit oral pathogen growth, opening new possibilities for shelf-stable product formulations.
Synbiotic Formulas: Combining Prebiotics and Probiotics Effectively
A synbiotic is a product that contains both probiotics and the prebiotics that specifically support them. In the oral health context, a formula combining S. salivarius M18 with inulin or arginine represents a synbiotic approach. The prebiotic creates a favorable environment for probiotic colonization while the probiotic displaces pathogenic species. This combination strategy is gaining traction in clinical research and represents the next generation of oral health supplementation.

How to Choose the Best Oral Probiotic Product in 2026
The oral probiotic market has grown exponentially. More than 25 companies now market oral health probiotic products in the United States, with over 50 bacterial species and strains included across formulations. Not all of them deliver what they promise. Here is how to evaluate any product rigorously.
📋 Checklist: How to Evaluate an Oral Probiotic Supplement
Before choosing any oral probiotic supplement, verify that it offers:
✅ Strain-level identification on the label (e.g., S. salivarius BLIS M18, not just “Streptococcus salivarius“)
✅ Adequate CFU quantity — minimum 1 billion, ideally 3–5 billion per dose
✅ Delivery format suited for oral use (lozenges or chewable tablets preferred over swallowed capsules)
✅ Clinical evidence specific to the oral cavity — not just gut health studies
✅ GMP certification and third-party testing for purity and potency
✅ Transparent ingredient list with dosages for each active strain
✅ Absence of artificial additives, aggressive preservatives, or unnecessary fillers
✅ Satisfaction guarantee (minimum 30 days, ideally 60 days)
✅ Manufacturer transparency — accessible scientific references, not just marketing claims
CFU Count: How Much Is Enough for Oral Benefits?
Colony-forming units (CFUs) indicate the number of viable bacteria per dose. For oral health benefits, clinical studies generally use doses between 1 billion and 10 billion CFU. A product with fewer than 1 billion CFU per dose is unlikely to establish meaningful colonization against the existing oral microbiome. However, more is not always better — strain viability, adhesion capacity, and appropriate delivery format matter as much as raw CFU numbers.
Delivery Format: Lozenges vs Capsules vs Chewables
This distinction is often overlooked but critically important. Swallowed capsules deliver probiotics to the gut, where they may benefit digestion but have minimal direct impact on the oral cavity. Lozenges and chewable tablets allow the probiotic bacteria to dissolve slowly in the mouth, making extended contact with oral tissues, teeth, and gum pockets. For any condition specifically targeting the oral microbiome — cavities, gum disease, bad breath — lozenges or chewables are the scientifically appropriate delivery format.
Shelf Stability and Strain Viability at Room Temperature
Many probiotic products lose significant CFU counts between manufacturing and consumption. Look for products that specify viability at the time of consumption (not just at manufacture), use microencapsulation technology, or include spore-forming strains like Bacillus coagulans that are inherently stable. Refrigerated storage extends shelf life for sensitive strains but can be inconvenient for daily compliance.
Third-Party Testing and GMP Certification: What to Look For
Good Manufacturing Practice (GMP) certification indicates that a product is produced under standardized quality control conditions. Third-party testing — by independent laboratories, not the manufacturer — provides an additional layer of verification for label accuracy and the absence of contaminants. In the United States, the FDA does not pre-approve dietary supplements; the burden of proof lies with the manufacturer and, ultimately, the consumer. Third-party certification is therefore the most reliable signal of product quality.
Top Oral Probiotic Products Compared: Strain Profiles and Evidence
Hyperbiotics PRO-Dental: Strains, Dosage, and Clinical Backing
Hyperbiotics PRO-Dental contains S. salivarius K12 and M18, L. reuteri, and L. paracasei in a time-release tablet format. The inclusion of both BLIS strains — the two most clinically supported oral probiotic strains — gives this product a strong evidence base for bad breath management and moderate support for gum health. The time-release format is designed to extend oral contact time, though independent verification of this claim is limited.
ProBiora3: Formulation Strengths and Ideal User Profile
ProBiora3 contains three strains isolated directly from healthy human oral tissue: S. oralis KJ3, S. uberis KJ2, and S. rattus JH145. All three were originally isolated and studied by Dr. Jeffrey Hillman beginning in 1985. This product has the most rigorous origin story of any oral probiotic on the US market — each strain was specifically selected for oral colonization, hydrogen peroxide production, and competitive exclusion of periodontal pathogens. It is the only commercial product built entirely around strains validated specifically for the oral cavity from the beginning.
Products Featuring BLIS M18: What the Research Supports
S. salivarius M18 — marketed under the BLIS M18 identifier — is one of the most commercially prominent oral probiotic strains. Products from BLIS Technologies, Hyperbiotics, and several other manufacturers include this strain. The research backing for M18 is strong: multiple randomized controlled trials demonstrate reductions in caries risk, periodontal pathogen counts, and gum inflammation. When evaluating any product claiming BLIS M18 inclusion, confirm that the strain identifier appears explicitly on the label.
What Makes ProDentim’s Probiotic Blend Scientifically Notable
ProDentim is a chewable tablet formulation designed specifically for oral cavity delivery. Its blend includes 3.5 billion CFU per dose, combining Lactobacillus Paracasei, Lactobacillus Reuteri, and Bifidobacterium lactis BL-04 alongside complementary ingredients including inulin (prebiotic), malic acid (enamel support and whitening), tricalcium phosphate (mineral reinforcement), and peppermint. The chewable format ensures direct contact with oral surfaces — the scientifically appropriate delivery mechanism for oral microbiome intervention.
The combination of probiotic strains with prebiotic (inulin) support reflects a synbiotic design philosophy. The inclusion of malic acid and tricalcium phosphate addresses enamel health in addition to microbial balance — a more comprehensive approach than probiotic strains alone. ProDentim is manufactured in FDA-registered, GMP-certified facilities and comes with a 60-day satisfaction guarantee, which meets the quality criteria outlined in the evaluation checklist above.
🎯 Want to learn more about ProDentim’s formulation and see whether it aligns with your oral health goals? Explore the official ProDentim page for complete ingredient transparency and clinical references →

How to Increase Good Bacteria in Your Mouth Naturally
Probiotic supplementation is most effective when supported by lifestyle and dietary habits that favor beneficial oral bacteria. Several everyday factors either nourish or deplete the commensal microbial population.
Dietary Choices That Support a Healthy Oral Microbiome
Fermented foods — yogurt with live cultures, kefir, and certain aged cheeses — introduce beneficial bacteria to the oral cavity transiently. Fibrous vegetables stimulate saliva flow, which mechanically cleans teeth and delivers antimicrobial compounds. Arginine-rich foods (legumes, seeds, whole grains) support the ADS pathway in commensal streptococci, raising oral pH. Conversely, frequent sugar consumption — particularly simple carbohydrates — provides the primary fuel for S. mutans and disrupts the ecological balance of the oral microbiome.
Habits That Destroy Beneficial Oral Bacteria
Smoking is one of the most damaging behaviors for the oral microbiome — it reduces oxygen levels in gum tissue (favoring anaerobes), impairs immune response, and dramatically alters microbial community composition. Chronic stress elevates cortisol, which suppresses salivary antimicrobial proteins and alters the immune environment in the gingival sulcus. Frequent antibiotic use eliminates large portions of both beneficial and pathogenic oral bacteria indiscriminately, often taking weeks or months for the microbiome to recover.
How Antiseptic Mouthwash Affects Microbial Balance
This is one of the most important and underappreciated points in oral microbiome science. Chlorhexidine and alcohol-based antiseptic mouthwashes are highly effective at reducing bacterial counts — including both pathogens and beneficial bacteria. Regular long-term use can reduce salivary nitrite-producing bacteria, which play a key role in cardiovascular health via the nitric oxide pathway. If using an oral probiotic, it is advisable to avoid antiseptic mouthwash use immediately before or after probiotic administration to avoid eliminating the introduced beneficial bacteria before they can colonize.
Combining Probiotic Supplements With Lifestyle Changes
Probiotic bacteria establish more readily in a favorable microbiome environment. Reducing dietary sugar, maintaining consistent mechanical cleaning (brushing and flossing), stimulating saliva flow through adequate hydration, and limiting antiseptic mouthwash use all create conditions in which introduced probiotic strains are more likely to colonize successfully and sustain populations over time.
How to Use Oral Probiotic Lozenges Correctly for Best Results
Even the best probiotic strains will underperform if used incorrectly. The following guidance is based on clinical study protocols and manufacturer recommendations from the most rigorously tested products.
Best Time of Day to Take Oral Probiotic Supplements
The optimal time for oral probiotic use is after brushing teeth — ideally at night before bed. This timing allows the probiotic bacteria maximum contact time with oral surfaces without immediate disruption from eating, drinking, or mouthwash. Morning use after brushing is also effective. The key principle is to avoid eating, drinking (anything other than water), or using mouthwash for at least 30 minutes after taking the probiotic.
How Long Until You Notice Oral Health Improvements?
Clinical studies consistently report that measurable changes in oral bacterial populations begin within two to four weeks. Subjective improvements in breath freshness often occur earlier — sometimes within one to two weeks. Gum health improvements, including reduced bleeding on probing and decreased inflammation, typically require four to eight weeks of consistent use. Enamel-related benefits, such as reduced sensitivity and gradual whitening, develop over longer periods — typically 60 to 90 days.
Expected Results at 30, 60, and 90 Days of Consistent Use
| Time Period | Expected Changes |
|---|---|
| Week 1–2 | Fresher breath, initial reduction in VSCs |
| Month 1 (30 days) | Reduced gum bleeding, improved salivary bacterial balance |
| Month 2 (60 days) | Decreased plaque accumulation, reduced sensitivity |
| Month 3 (90 days) | Measurable gum tissue improvement, gradual enamel support |
Individual results vary based on baseline oral health, diet, hygiene habits, and strain-specific colonization capacity. These timeframes reflect averages from clinical trial data rather than guaranteed outcomes.
Can You Take Oral Probiotics Alongside Antibiotics?
Antibiotics — both systemic and topically applied in the mouth — significantly reduce probiotic bacterial counts. If you are prescribed oral antibiotics, it is advisable to complete the antibiotic course before resuming or beginning oral probiotic supplementation. Separating antibiotic and probiotic doses by at least two hours can reduce interference in cases where concurrent use is unavoidable. Always consult your dentist or physician before combining supplements with prescription medications.
Compatibility With Other Dental Care Products
Standard fluoride toothpaste, floss, and non-antiseptic mouthwashes are fully compatible with oral probiotic use. Water flossers and tongue scrapers — which mechanically remove biofilm — do not chemically interfere with probiotics and can enhance their effectiveness by clearing space for beneficial colonization. The primary compatibility concern is antiseptic mouthwash, as discussed above.
Who Should and Should Not Use Oral Probiotic Strains
Most adults can safely use well-characterized oral probiotic strains. However, certain populations require additional consideration.
Ideal Candidates: Conditions That Benefit Most
Individuals most likely to benefit from oral probiotic supplementation include those with recurrent cavities or persistent plaque despite good hygiene, chronic or recurrent gingivitis, chronic halitosis not resolved by standard hygiene, a history of antibiotic use that has disrupted the oral microbiome, dry mouth (xerostomia, which reduces natural antimicrobial saliva protection), and those seeking a proactive preventive approach to long-term dental health.
Pregnant Women, Children, and Immunocompromised Individuals
GRAS-status probiotic strains — including S. salivarius K12, M18, and the ProBiora strains — have strong safety records. However, pregnant women, children under two, and immunocompromised individuals (including those undergoing chemotherapy or taking immunosuppressant medications) should consult a healthcare provider before beginning any probiotic supplementation. This is a general precaution standard for all dietary supplements, not a specific concern unique to oral probiotics.
Potential Drug Interactions and When to Consult a Dentist
No clinically significant drug interactions have been identified for the oral probiotic strains reviewed here. However, individuals taking blood thinners, systemic antifungals, or immunosuppressants should disclose supplement use to their physician. Any new supplement — including oral probiotics — should be discussed with a dentist, particularly for patients with active periodontal disease, recent dental surgery, or implants.
Common Myths About Oral Probiotics Debunked
“Probiotics Can Replace Brushing and Flossing” — True or False?
False. Oral probiotics are an adjunct to mechanical oral hygiene — not a replacement. Brushing removes biofilm mechanically; flossing disrupts interproximal plaque that brushes cannot reach. Probiotics work at the microbial level, shifting bacterial community composition over time. Neither strategy is effective without the other. Clinical trials on oral probiotics consistently use mechanical hygiene as a baseline — probiotic effects are measured on top of standard care.
“All Probiotics Are the Same” — Why Strain Specificity Matters
False. This is perhaps the most consequential misconception in the oral probiotic market. A Lactobacillus acidophilus strain optimized for gut colonization has no documented oral cavity benefit — and research actually implicates L. acidophilus in caries progression. Conversely, S. salivarius M18 — isolated from human oral tissue and validated in multiple dental clinical trials — delivers consistent, strain-specific benefits. The species name tells you almost nothing. The strain identifier tells you everything.
“More CFUs Always Means Better Results” — What Science Says
False. Colonization success depends on adhesion capacity, strain viability at the time of consumption, the existing microbiome composition, and delivery format — not CFU count alone. A 1-billion CFU lozenge of S. salivarius K12 will outperform a 50-billion CFU capsule of L. acidophilus swallowed whole for oral cavity benefits. Quality and strain selection trump quantity every time.

Scientific Research on Oral Probiotic Strains: Key Studies
The evidence base for oral probiotics has grown substantially in the past decade. Several landmark studies deserve specific mention for consumers and clinicians evaluating the field.
Randomized Controlled Trials on Lactobacillus for Gum Health
A 2020 randomized controlled trial published in the Journal of Periodontology found that sailors consuming L. reuteri-containing lozenges for 12 weeks showed significant improvements in gingival index and plaque index compared to placebo. A 2020 clinical trial by Laleman et al. in Journal of Clinical Periodontology found mixed results — improving some periodontal parameters while leaving others unchanged — reflecting the importance of strain and study design in interpreting outcomes.
Clinical Evidence on Streptococcus Salivarius for Oral Hygiene
The clinical evidence for S. salivarius K12 and M18 is the most consistent in the oral probiotic field. A 2022 randomized controlled trial in Cureus demonstrated that K12 and M18 lozenges significantly reduced cariogram risk parameters in high-caries-risk patients over 90 days. A 2021 study by Jansen et al. in PLOS ONE confirmed that a combination of probiotic strains including S. salivarius concertedly inhibited periodontitis-associated bacteria in clinical samples.
Limitations of Current Research and What Studies Are Missing
Despite growing evidence, important gaps remain. Most clinical trials are short-term (less than 12 weeks), involve small sample sizes, and focus on surrogate markers (bacterial counts, bleeding scores) rather than hard clinical endpoints (tooth loss, bone level preservation). Long-term safety data beyond six months is limited for most strains. Additionally, studies on vulnerable populations — the elderly, children, and immunocompromised patients — are underrepresented. Future research should also address optimal dosing regimens, ideal combination formulas, and the interaction between oral probiotics and systemic conditions such as diabetes and cardiovascular disease.
Frequently Asked Questions About Oral Probiotic Strains
What are the best probiotic strains specifically for oral health?
The strains with the strongest clinical evidence are S. salivarius BLIS M18 (cavities, gum disease), S. salivarius K12 (bad breath), S. oralis KJ3 / S. uberis KJ2 (periodontal pathogens), and L. paracasei (plaque biofilm). Strain-level identification on the label is essential.
How do oral probiotics differ from digestive probiotic supplements?
Oral probiotics are isolated from human oral tissue and adapted to colonize the mouth. Gut probiotics are optimized for intestinal survival. Swallowing gut probiotics provides no meaningful oral cavity benefit — the delivery format (lozenge vs capsule) also determines where the bacteria are released.
How long does it take for oral probiotics to show results?
Breath improvements often appear within one to two weeks. Measurable gum health changes typically require four to eight weeks. Enamel-related benefits and significant microbiome rebalancing are usually observed after 60 to 90 days of consistent daily use.
Can oral probiotics help with gum disease or periodontitis?
Yes, as an adjunct to professional care. Several RCTs show that probiotic strains — particularly S. salivarius M18 and L. reuteri — reduce periodontal pathogen counts and gingival inflammation. They do not replace scaling, root planing, or surgical treatment for advanced periodontitis.
Are probiotic lozenges more effective than probiotic capsules for teeth?
Yes, for oral cavity benefits. Lozenges dissolve in the mouth, allowing extended contact between probiotic bacteria and oral surfaces, teeth, and gum tissue. Swallowed capsules bypass the oral cavity and deliver probiotics to the gut, providing no direct dental benefit.
Is it safe to take oral probiotics every day long-term?
All GRAS-status oral probiotic strains — including S. salivarius K12 and M18 — have excellent long-term safety profiles with no serious adverse events reported in clinical literature. However, consultation with a healthcare provider is recommended for immunocompromised individuals or those on multiple medications.
Can children use oral probiotic strains safely?
Yes, with appropriate guidance. S. salivarius M18 has been studied specifically in children in caries prevention trials with no adverse effects. Lower-dose formulations designed for children are available. Parents should consult a pediatric dentist before beginning supplementation in children under five.
Do oral probiotics help whiten teeth naturally?
Some probiotic formulations include malic acid, which stimulates saliva and gently removes surface stains. Additionally, low-level hydrogen peroxide produced by S. oralis KJ3 has a documented mild whitening effect on enamel. Whitening is gradual and cosmetic — it results from a cleaner oral environment rather than chemical bleaching.
What is BLIS M18 and why is it important for dental health?
BLIS M18 is the commercial identifier for Streptococcus salivarius strain M18. It produces three distinct bacteriocins — salivaricin A2, salivaricin 9, and salivaricin M — that inhibit the bacteria responsible for cavities, gum disease, and plaque. Multiple RCTs support its efficacy, making it the most clinically validated oral probiotic strain currently available.
Should I stop using antiseptic mouthwash if I take oral probiotics?
You do not need to stop entirely, but timing matters. Avoid using antiseptic mouthwash immediately before or after taking an oral probiotic, as it will eliminate the introduced bacteria before they can colonize. A separation of at least 30 to 60 minutes is advisable. Consider whether daily antiseptic mouthwash use is necessary — for most people with standard oral hygiene, it is not recommended long-term.
Can oral probiotics reduce tooth sensitivity?
Indirectly, yes. By reducing acidic bacterial activity and supporting oral pH balance, probiotic strains can reduce the microenvironmental conditions that drive enamel erosion and dentin exposure. Products that combine probiotics with tricalcium phosphate and malic acid may provide additional mineral support for sensitive teeth.
Are Hyperbiotics PRO-Dental and similar products clinically validated?
Hyperbiotics PRO-Dental contains S. salivarius K12 and M18 — strains with strong clinical validation. The specific product formulation has not undergone independent clinical trials, but the included strains have been validated by multiple third-party research groups. Verifying strain identifiers on the label remains the most important quality check.
Do oral probiotics interact with antibiotics or dental medications?
Antibiotics significantly reduce probiotic effectiveness. Separate their use by at least two hours where possible, or resume probiotics after completing an antibiotic course. No significant interactions have been identified with standard dental medications (local anesthetics, topical fluoride, chlorhexidine gels), though timing around antiseptic agents should be managed as described above.
What should I look for on a probiotic label to ensure quality?
Look for: strain-level identification (e.g., S. salivarius BLIS M18, not just “Streptococcus”), CFU count at time of expiration (not just manufacture), GMP certification mark, third-party testing disclosure, and absence of artificial colors or preservatives. Manufacturer contact information and scientific references should be accessible and transparent.
Can pregnant or breastfeeding women take oral probiotic supplements?
GRAS-status strains are generally considered safe. However, no specific clinical trials on oral probiotics during pregnancy exist. The conservative recommendation is to consult a physician or dentist before beginning supplementation during pregnancy or breastfeeding. Maintaining excellent mechanical oral hygiene during pregnancy is especially important, as pregnancy hormones increase susceptibility to gingivitis.

Conclusion: Building a Smarter Oral Health Strategy in 2026
The science of oral probiotics has matured significantly. What began as a fringe concept in dentistry has now generated dozens of randomized controlled trials, a growing commercial market valued at over $100 million in North America alone, and genuine enthusiasm from dental professionals seeking proactive, microbiome-informed care strategies. The evidence is clear: the best probiotic strains for oral health — particularly S. salivarius BLIS M18, BLIS K12, S. oralis KJ3, and L. paracasei — offer measurable, scientifically grounded benefits for gum health, cavity prevention, and breath management.
However, not all probiotic products are equal. The oral health probiotic market is saturated with products containing gut bacteria at inadequate doses in inappropriate delivery formats — generating consumer confusion and warranting genuine skepticism. The guidance in this article empowers you to cut through marketing noise and evaluate any probiotic product against objective scientific criteria. Strain-level identification, appropriate CFU counts, oral-cavity delivery format, and third-party quality certification are non-negotiable.
For those looking to explore a comprehensive oral probiotic formulation that integrates evidence-supported strains with enamel-supporting ingredients in an appropriate chewable format, ProDentim represents a scientifically thoughtful option. As with any health supplement, consistent use over at least 60 to 90 days — alongside regular brushing, flossing, and professional dental care — provides the most meaningful foundation for lasting oral health.
🎯 Ready to take the next step in your oral health journey? Visit the official ProDentim page to review the complete formulation, ingredient transparency, and 60-day satisfaction guarantee →
📚 Recommended for You (50)
Adele Smith is a health and wellness researcher specializing in natural solutions for vision care, nutrition, and healthy aging.
For several years, she has studied the relationship between lifestyle, dietary supplements, and long-term eye health. Her work focuses on helping readers understand natural approaches that may support vision and promote overall wellness.
Through her articles, Adele shares research-based insights and educational health information designed to help readers make informed decisions about their well-being.